Efficacy of Painhunting Therapy for Event-Related Depression
 Olzhas Seitov
Olzhas Seitov
Abstract
A randomized controlled trial (NCT07490691, n = 84) demonstrated that Painhunting therapy — a brief course of three to four sessions — produces clinically significant reductions in depression in adults experiencing psychological distress related to an adverse life event. Two weeks after the start of treatment, the mean PHQ-9 score in the therapy group was 2.32 versus 16.56 in the waitlist group (effect size Cohen d = 2.78; p < 0.001); 79% of participants achieved remission. The effect was independently replicated: the waitlist group, upon crossing over to treatment, showed an identical reduction in symptoms. At eight weeks — approximately one month after completing therapy — results remained stable, with 68% of participants maintaining remission. Anxiety, complicated grief, and functional disability measures improved in parallel. The study was conducted in Astana, Kazakhstan, approved by the al-Farabi KazNU Ethics Committee, and data are openly available on OSF (osf.io/s8h74).
Keywords
Research Type
- Randomized Controlled Trial
In 2026, a randomized controlled trial (RCT) of the Painhunting method was completed — the most rigorous standard for evaluating psychotherapeutic interventions. The study is registered in the international clinical trial database ClinicalTrials.gov (NCT07490691), approved by the al-Farabi KazNU Ethics Committee, and was conducted under the supervision of independent Principal Investigator Sanemkhan Uzakova. Below is what was studied, how it was conducted, and what the results showed.
Why Conduct Such a Study
Painhunting has been practiced for over eight years, with more than 500 trained specialists and over 10,000 client sessions conducted. But personal experience is not evidence. People recover for many reasons: time, support from loved ones, simply talking to someone attentive. To separate the effect of the method from everything else, a control group is required.
A randomized controlled trial is when participants are randomly divided into two groups: some receive treatment immediately, others wait. If after two weeks the first group feels significantly better and the second does not, that is the effect of the method — not spontaneous recovery.
Who Participated
198 people applied to the trial. After screening and psychometric assessment, 84 participants were admitted — all with clinically significant depression (PHQ-9 ≥ 9) and a clearly identified adverse life event underlying their condition: bereavement, divorce, serious illness, financial crisis, and other distressing circumstances.
Participants were randomly assigned:
- Group A (42 participants) — immediately began Painhunting therapy
- Group B (42 participants) — two-week waitlist, then also received therapy
Mean age was 42 years; 89% of participants were women. Baseline depression levels were virtually identical across both groups.
How Therapy Was Delivered
Each Group A participant completed three Painhunting sessions over two weeks (a fourth was added if symptoms persisted). Each session lasted 90–120 minutes. Six certified specialists delivered the intervention, with career experience ranging from 95 to 3,657 sessions.
Group B remained on the waitlist during this period — no therapeutic sessions, only weekly safety check-ins. After the control period ended, Group B also completed the full course of therapy.
What Was Measured
Four clinically validated instruments — all internationally recognized:
- PHQ-9 — depression scale (primary outcome)
- ICG — Inventory of Complicated Grief
- GAD-7 — generalized anxiety scale
- WHO-DAS 2.0 — functional disability in daily life
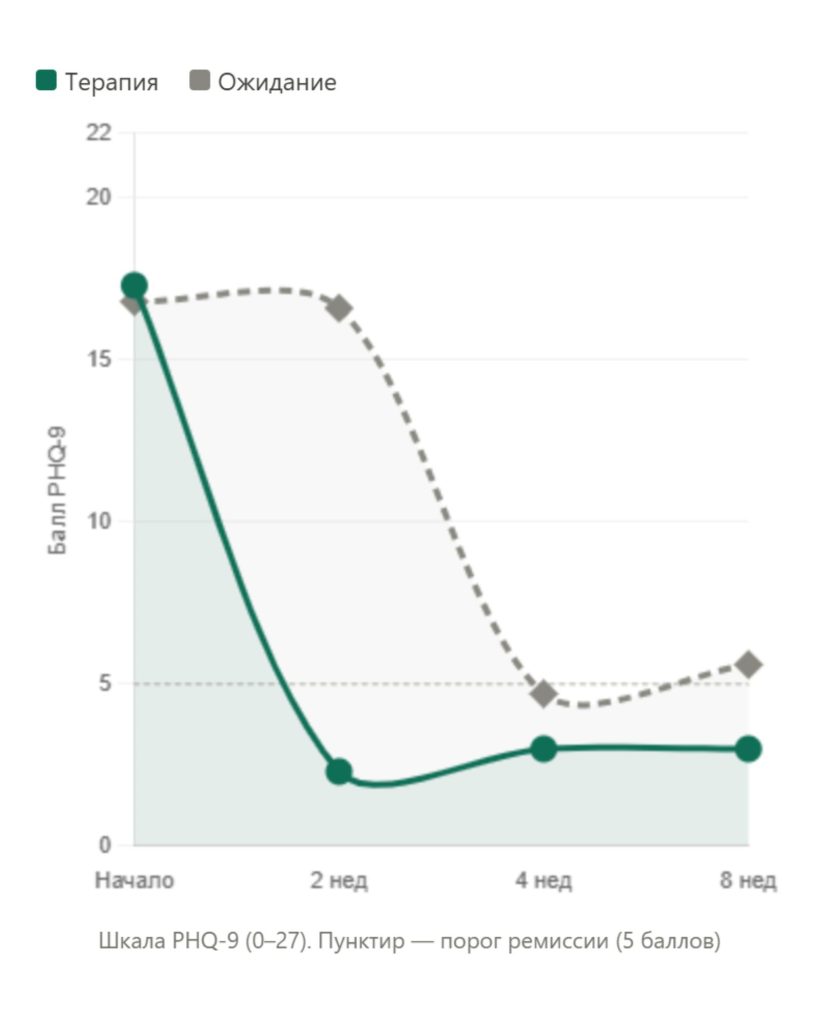
Assessments were conducted at four time points: before therapy, at two weeks, at four weeks, and at eight weeks after the start of the study.
Results
After Two Weeks: The Gap Between Groups
After two weeks, the mean PHQ-9 score in Group A was 2.32 — the “minimal symptoms” range, essentially normal. In Group B, which had been waiting throughout, it was 16.56, nearly unchanged from baseline.
The difference of 14.25 points is statistically highly significant (p < 0.001). The effect size — Cohen d = 2.78 — is three to four times higher than the average typically observed in psychotherapy research for depression.
For reference: in the largest meta-analysis of psychotherapy for depression (Cuijpers et al., 2018, 385 studies), the mean effect relative to waitlist control was d = 0.72.
Internal Replication: Group B Achieved the Same Result
After Group B completed therapy, its result reproduced Group A’s result to within half a point: PHQ-9 reduction of 14.19 versus 14.71. This is an internal replication of the effect in a separate subgroup at a different time point — an important argument that the result was not due to chance.
What Happened in the Waitlist Group
Over the two-week wait, Group B showed virtually no change: PHQ-9 increased by 0.22 points (p = 0.81). This rules out the “it got better on its own” explanation — symptoms do not resolve over time without treatment.
Remission
Remission is defined as PHQ-9 < 5 — a return to normal. After two weeks of therapy, 79% of Group A participants achieved remission. For comparison: in the waitlist group, remission occurred in only 3%.
Anxiety, Grief, and Daily Functioning
Alongside depression, all other measures improved:
- Complicated grief (ICG): reduction of ~30 points
- Anxiety (GAD-7): reduction of ~9.5 points
- Functional disability (WHO-DAS): reduction of ~12 points
The same pattern was observed in Group B after crossing over to treatment.
Durability of Effect at Eight Weeks
Eight weeks after the start of the study — four weeks after the end of therapy — Group A was reassessed. Result: PHQ-9 = 2.97, change from the previous time point: +0.05 points. Essentially unchanged. 68% of Group A participants remained in remission one month after completing the course.
This is not a temporary mood lift following a session — it is a durable change.
How Reliable Are These Results
Several factors increase confidence in the data:
- Dual replication within a single study. Both groups achieved comparable effects at different times and independently of each other.
- Flat control. The waitlist group showed no improvement — ruling out natural recovery as an explanation.
- Four independent measures moved in the same direction simultaneously. Bias in any one instrument could not have produced this pattern.
- Expectations and personal factors do not explain the result. Analysis showed that therapeutic alliance, treatment credibility, self-efficacy, age, and sex had near-zero associations with outcome.
- Independent blinded re-assessment. 20% of Group A participants were re-interviewed by telephone by an independent assessor blinded to their self-report data. Correlation with self-reports: r = 0.88.
Limitations
The study was transparent and openly acknowledged its limitations:
- Single site (Astana), predominantly female sample — results may not fully generalize to other contexts.
- Dropout in the waitlist group was higher than in the therapy group (expected in a waitlist-controlled design).
- The study was conducted without external funding, and the method’s developer participated in the process.
- No active comparator — CBT or another established therapy. This is the objective of the next study (RCT #2: Painhunting versus CBT).
Acknowledging these limitations is not a weakness — it is a mark of honest science. They have already been incorporated into the protocol for the next study.
What Comes Next
The first RCT answers the question: “better than nothing?” — and the answer is compelling. The next step is RCT #2: a direct comparison of Painhunting against manualized cognitive-behavioral therapy in a randomized design. The protocol is already in development.
Preprint and Open Data
The full scientific paper with data, tables, and statistical analysis is published in open access on medRxiv:
Link: https://www.medrxiv.org/lookup/content/short/2026.06.08.26355224v1
Study data are openly available on the Open Science Framework: osf.io/s8h74
Trial registration on ClinicalTrials.gov: NCT07490691
How to Cite
Seitov O, Bayat V, Uzakova S. Efficacy of Painhunting Therapy for Adverse-Event-Related Depression. medRxiv 2026.06.08.26355224; doi: https://doi.org/10.64898/2026.06.08.26355224


